Sympathetic Ophthalmitis (SO) is defined as a bilateral
granulomatous uveitis of unknown etiology, occurring after penetrating trauma
or intraocular surgery. It is believed to represent a form of autosensitization
of ocular tissue following a perforating injury to one eye. Its exact incidence
is not known but is thought to be 1.9% after trauma and 0.007% after
intraocular surgery1.
SO is an uncommon disease due to improved surgical techniques
employed in the repair of ocular injuries and early enucleation of the blind
eye. The risk of developing SO in severely traumatized eyes with no visual
potential that are not enucleated is exceedingly low2.
Numerous surgical procedures such as 23-guage vitrectomy3,
cataract extraction4, retinal detachment surgery5,
penetrating keratoplasty6 and trabecule-ctomy7 have been
complicated by SO.
We report a case of SO seen in our outpatient department (OPD) at
Isra Postgraduate Institute of Ophthalmology / Al-Ibrahim Eye Hospital,
Karachi.
CASE REPORT
A 30 year old male, plumber by profession was seen in OPD with
complaint of gradual painful loss of vision in his right eye of 10 days
duration. About 25 days back, this patient sustained penetrating trauma to his
left eye with a piece of wood. The patient did not have any significant medical
and surgical history. On examination, his best corrected visual acuity (BCVA)
was Hand movements (HM) in right eye and no perception of light (NPL) in left
eye. His right eye, on biomicroscopic examination showed multiple mutton-fat
keratic precipitates (KPs) with 2-3 plus cells and flare in the anterior
chamber (Fig. 1 & 2).The pupil was fixed and dilated with multiple
posterior synechie (PS) formation. The intraocular pressure (IOP) measured 12
mm Hg. The fundus examination revealed optic disc edema and serous retinal
detachment (Fig. 3). The patient’s left eye was pthysical with vertical full
thickness corneal laceration (Fig. 4). The patient went under laboratory
investigations of complete blood count (CBC), erythrocyte sedimentation rate
(ESR), rapid plasma regain (RPR), venereal disease research laboratory (VDRL),
fluorescent treponemal antibody absorption test (FTA – ABS), toxoplasmosis IgG
and IgM, angiotensin converting enzyme (ACE) and antinuclear antibody (ANA)
test. Patient also had X-ray chest, B-Scan (Fig. 5), fundus flourescein
angiography (FFA), (Fig. 6) and optical coherence tomography (OCT). All
laboratory tests including X-ray chest were within normal limits. A clinical
diagnosis of SO was entertained and patient was commenced on tablet
prednisolone 60 mg / day in divided doses (1 mg / kg body weight), prednisolone
1% drops (Predforte- Allergan, Pakistan), several times a day and atropine 1%
twice a day (Ophth-Atropine - Ophth, Pakistan).
At two weeks patient’s vision had improved to 6/24 with anterior
chamber getting quite and reduction in the number of KPs. The optic disc
margin, though still appeared blurred but swelling had subsided significantly.
Subretinal serous fluid also had decreased with B-Scan appearing normal.
Patient’s systemic and topical treatment continued.
At four week follow up,
patient’s BCVA appeared stable at 6/18 on Snellen’s quotations.
DISCUSSION
The etiology of SO has not been completely understood, but the
underlying pathophysiology is believed to be an autoimmune reaction against the
exposed ocular antigens from the inciting eye8. The location of such
antigens remains controversial and may be found in the uveal tissue, retina or
choroidal melanocytes. The immunologic studies have shown CD4 helper and
inducer T cells during the early phase of inflammation compared to infiltration
by CD8 suppressor and cytotoxic T cells in the later stage. There are B
lymphocytes also found in some patients9.
Lymphocytes from patients with SO were demonstrated to respond to
several uveo-retinal antigens. Although no circulating antiretinal S-antigen
antibodies were found, the serum from patients with SO showed antiretinal
antibodies directed against the outer segment of photoreceptors and the Muller
cells, when placed over normal human retinal tissue10.
It has also been hypothesized that a purulent infection within the
eye would destroy the uveal tissue in such a way that SO would not develop.
However some cases have been reported in eyes with endophthalmitis or fungal
keratitis, indicating that the infection may not offer any prevention against
development of SO11.
The SO can occur between two weeks and three months after an
ocular injury, although it can develop as early as several days and as late as
50 years, majority of cases present within first three months. Classically, the
inflammation is granulomatous with multiple mutton-fat KPs adhered to corneal
end-othelium. The iris can be thick and sticky with PS formation. The IOP can
be normal or fluctuating upwards or downwards due to the inflammatory
involvement of ciliary body and trabecular meshwork. The vitreous is usually
infiltrated with moderate to severe cellular reaction. The fundus can show
swollen optic disc and multiple yellow-white lesions in the periphery,
corresponding to the presence of Dalen-Fuchs nodules, which may not be seen in
almost 50% of the cases. Serous retinal detachment or macular edema may be
present with subretinal neovascu-larization.
On fundus flourescein angiography (FFA), the optic nerve head
shows hyperemia and dye leakage more pronounced in the late frames. There are
multiple hyperflourescent areas of choroidal leakage corresponding to the
presence of Dalen-Fuchs nodules. The less common appearance on FFA is that of
early hyperflourescent lesions with staining in the late phase. This type of
picture is thought to be related to whether the Dalen-Fuchs nodules have an
intact or disrupted over lying retinal pigment epithelium (RPE)12.
Extra ocular findings such as pleocytosis of cerebro-spinal fluid,
hearing loss, alopecia, poliosis and vitiligo have been reported with SO,
although these findings are more common in Vogt Koyanagi Harada (VKH) disease.
The sequelae of the ocular inflammation include secondary
glaucoma, cataract, optic atrophy, retinal detachment with subretinal fibrosis
and choroidal atrophy.
SO is characterized by a diffuse granulomatous, non-necrotizing
inflammation involving entire uveal tract. The choroid is thickened with
lymphocytic infiltration along with the presence of eosinophils and plasma
cells. Typically, the choriocapillaris is spared. The Dalen-Fuchs nodules
representing migrated and transformed RPE cells are typical but not
pathagnomonic and may be present in other disease such as: VKH syndrome. These
nodules are collection of epitheloidhistocytes and lymphocytes, present between
RPE and Bruch’s membrane13,14.

Fig. 1. Multiple mutton-fat keratic precipitates in right eye

Fig. 2. Multiple
mutton-fat keratic precipitates in right eye seen with slit beam

Fig. 3. Swollen optic disc and serous
retinal detachment in right eye
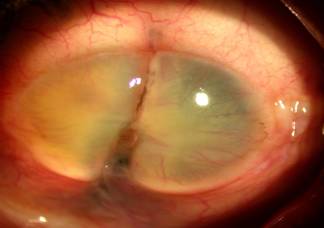
Fig. 4. Severe
lacerated cornea with pthysical left eye

Fig. 5. Serous retinal
detachment in right eye on Ultrasonic B-scan
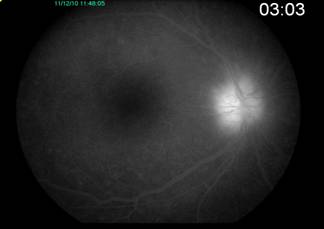
Fig. 6. Hyperfluorescent
disc in late venous phase in right eye
It is important to rule out the other causes of granulomatous
uveitis before a diagnosis of SO can be entertained. Although diagnosis of SO
is clinical, histopathology can be confirmatory. Autoimmune disease like VKH,
sarcoidosis, and multifocal choroiditis can have similar presentation.
Intraocular lymphoma and bilateral phacoanaphylaxis can also have a similar
picture. Infections like tuberculosis and syphilis should always be excluded.
SO is a rare but a significant complication of penetrating ocular
injury. In addition to systemic and intravitreal steroid therapy,
immunosuppressive drugs also play a significant role in the medical management
of this disease. The patient’s medical treatment needs to be carefully
monitored to reduce any side effects and improve visual prognosis.
Author’s affiliation
P. S. Mahar
Isra Postgraduate Institute
of Ophthalmology
Karachi
Aimal Khan
Isra Postgraduate Institute
of Ophthalmology
Karachi
Dilshad Laghari
Isra Postgraduate Institute
of Ophthalmology
Karachi
Sadaf Ambreen
Isra Postgraduate Institute
of Ophthalmology
Karachi
REFERENCE
1.
Liddy
BSL, Stuart J. Sympathetic Ophthalmitis in Canada. Can J Ophthalmol. 1972; 7:
157-60.
2.
Brackup
AB, Carter KD, Nerad JA et al. Long term follow up of
severely injured eyes following globe rupture. Ophthalmic Plast Reconstr Surg.
1991; 7: 1994-7.
3.
Cha DM,
Woo SJ, Ahn J, et al. A case of sympathetic Ophthalmia presenting with extraocular
symptoms and conjunctival pigmentation after repeated 23-guages vitrectomy.
Ocular ImmunalInflamm. 2010; 18: 265-7.
4.
Kinyoun
JL, Bensinger RE, Chuang EL. Thirty year history of sympathetic
ophthalmia. Ophthalmol. 1983; 90: 59-62.
5.
Wang WJ.
Clinical and histopathalogical report of sympathetic ophthalmia after retinal
detachment surgery. Br J Ophthalmol. 1983; 67: 150-2.
6.
Maheshwari
S, Rao V. Sympathetic ophthalmia following therapeutic penetrating
keratoplasty. Asian J Ophthalmol. 2007; 9: 89-91.
7.
Shammas
HF, Zubyk NA, Stanfield TA. Sympathetic Uveitis following glaucoma
surgery. Arch Ophthalmol. 1977; 95: 638-41.
8.
Kilmartin
DJ, Dick AD, Forrester JV. Sympathetic Ophthalmia risk following
vitrectomy. Should we council patients. Br J Ophthalmol. 2000; 84: 448-9.
9.
Shah DN,
Piacentini MA, Burnier MN, et al. Inflammatory cellular kinetics
in sympathetic ophthalmia: A study of 29 traumatized (exciting) eyes.
OculImmunolinflamm 1993; 1: 255-62.
10.
Chan CC,
Palestine AG, Nussenblatt RB, et al. Anti-retinal auto antibodies
in Vogt-Koyanagi-Harada syndrome, Behcet’s disease and sympathetic ophthalmia.
Ophthalmology. 1985; 92: 1025-8.
11.
Rathinam
SR, Rao NA. Sympathetic ophthalmia following postoperative bacterial
endophthalmitis: A clinicopathologic study. Am J Ophthalmol. 2006; 141:
498-507.
12.
Sharp
DC, Bell RA, Patterson E, et al. Sypmpathetic Ophthalmia,
histopathalogic and angiographic correlation. Arch Ophthalmol. 1984; 102:
202-35.
13.
Jakobiec
FA, Marboe CC, Knowles DM, et al. Human sympathetic ophthalmia:
an analysis of the inflammatory infiltrate by hybridoma-monoclonal antibodies,
immunoche-mistry, and correlative electron microscopy. Ophthalmology. 1983; 90:
76-95.
14.
Chan CC,
BenEzra D, Rodrigues MM, et al. Imunohistochemisty and electron
microscopy of choroidal infiltrates and Dalen-Fuchs nodules in sympathetic
ophthalmia. Ophthalmology. 1985; 92: 580-90.